111-29 Queens Blvd, Forest Hills, NY 11375
111-29 Queens Blvd, Forest Hills, NY 11375
![]()
![]()
Atypical lymphocytosis is an increase in lymphocytes that may appear unusually large or activated on a blood smear. It is most commonly caused by reactive immune responses to infections (especially EBV/mononucleosis and CMV), but persistent or unexplained cases may require evaluation for lymphoproliferative disorders such as CLL or lymphoma.
Lymphocytes are white blood cells that help your body fight infections and support immune memory.
A “high” lymphocyte count (lymphocytosis) in adults is commonly defined as an absolute lymphocyte count (ALC) > 4,000 cells/µL.
Some clinical pathways define “significant lymphocytosis” at ALC > 5 × 10⁹/L, especially when deciding who needs further workup.
Important: “Atypical lymphocytosis” is not a diagnosis by itself—it’s a lab pattern. The next step is figuring out why it’s happening.
You might see one or both on a lab report:
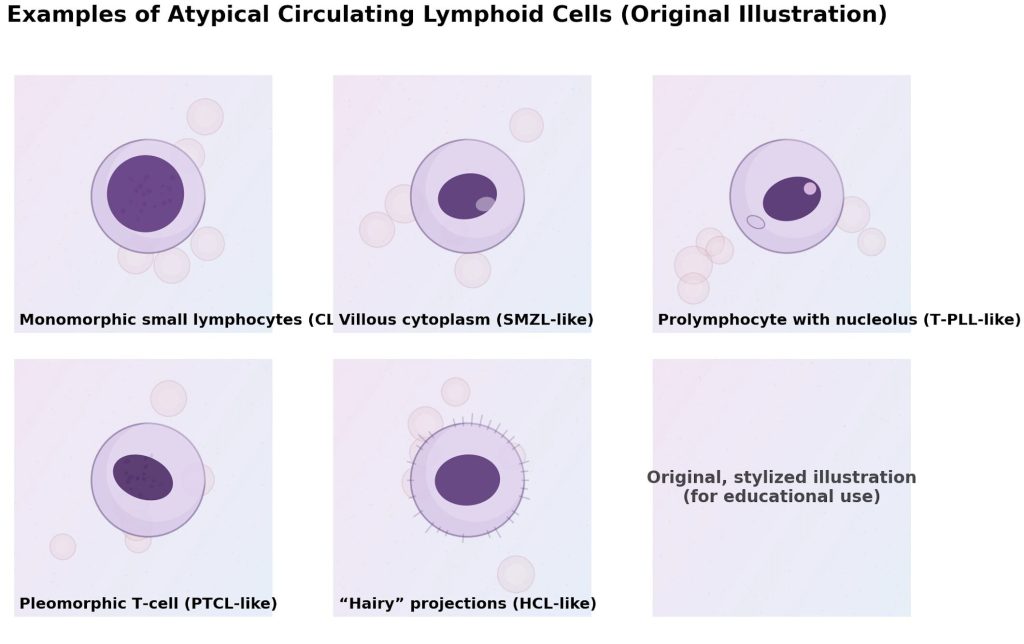
A smear review is helpful because reactive lymphocytosis tends to show a variety of lymphocyte appearances, while malignant lymphocytosis often looks more monomorphic (many cells look very similar).
Reactive (benign) lymphocytosis is frequently triggered by infection, inflammation, physiologic stress, or certain drug reactions. Examples include:
When lymphocytosis is persistent, unexplained, or accompanied by “red flags,” clinicians consider blood/lymphatic disorders such as:
A high lymphocyte count itself may not cause symptoms. Many people discover it incidentally on routine bloodwork.
When symptoms do happen, they usually relate to the underlying cause, such as:
Make an appointment promptly if you have atypical lymphocytosis plus any of the following:
Some guidance suggests that mild lymphocytosis lasting < 3 months in a well patient without other abnormalities often does not require extensive workup, but persistent unexplained lymphocytosis does.
At Medex, evaluation typically follows a practical sequence:
We re-check the CBC to confirm whether the abnormality is transient vs persistent and to look for other changes (anemia, platelet abnormalities).
Key questions include:
A smear can show whether lymphocytes appear reactive and diverse vs suspiciously uniform (more concerning).
Depending on symptoms, tests may include EBV/mono and other viral studies (clinically guided). EBV-related illness is a classic cause of atypical lymphocytes.
Flow cytometry helps determine whether lymphocytes are polyclonal (reactive) or monoclonal (suggesting a lymphoproliferative disorder). Clinical pathways note it is most informative when lymphocytosis is significant/persistent and the clinical picture warrants it.
Treatment depends entirely on the cause:
Atypical lymphocytosis is common and very often benign, especially after infections.
The goal is not to jump to worst-case scenarios—it’s to make sure the pattern fits a typical reactive process and to identify the smaller group of patients who need additional testing.
Request an appointment at Medex Diagnostic & Treatment Center to review your labs and symptoms and get a clear plan for follow-up.
This content is for educational purposes and does not replace personalized medical advice. If you have concerning symptoms or abnormal labs, please seek evaluation from a qualified healthcare professional.
Medex is a multi-specialty clinic with 24-hour urgent care, primary care, and more than 30 board-certified specialists, including podiatry, cardiology, dermatology, pain management, gynecology, and physical therapy. Each department works under one roof for seamless referrals.
Yes. Every Medex doctor is board-certified in their specialty, undergoes peer review, and participates in ongoing CME (continuing medical education). Credentials are listed on our Meet the Doctors page.
Absolutely. Our Queens urgent care clinic is open for walk-in patients with minor injuries or sudden illnesses. You can also save time by reserving a same-day slot online.
Medex accepts all major commercial carriers plus Medicare, Medicaid, HIP, EmblemHealth, MetroPlus, Fidelis, and GHI. For specific coverage questions, call (718) 275-8900 or visit our Insurance page.
Use our secure online booking portal, call (718) 275-8900, or log in to the Patient Portal to reschedule.
Yes—most primary care and follow-up visits can be conducted via HIPAA-compliant video. Sign the Telemedicine Consent Form and choose “Virtual” when booking.
Yes. Our No-Fault Doctor Queens team handles car- accident injuries, and our Workers’ Comp Clinic manages job-related injuries and paperwork.
We’re at 111-29 Queens Blvd, Forest Hills, NY 11375—steps from the Forest Hills–71 Av subway station (E, F, M, R lines). A paid garage is next door and metered street parking surrounds the building.
We follow HIPAA privacy rules, store EHR data on encrypted servers, and require two-factor authentication for staff access. You may request records through our ChartRequest portal.
Adults in good health should schedule an annual physical. Patients managing chronic conditions may need follow-ups every 3–6 months; your doctor will advise a personalized schedule.
For safety, we require an active chart and a visit within the past 12 months (3 months for controlled substances). Ask your pharmacy to send an electronic refill request or message us through the Patient Portal.
Last reviewed: March 22, 2026.